
Objective
After studying this chapter, you should be able to:
- Explain the importance of introducing a peripheral venous catheter;
- Demonstrate this procedure using a model or simulator in the laboratory and later in
clinical practice; - Name the basic types and parts of IV cannulas;
- Assess the risks of potential complications;
- Identify changes in the care of a peripheral venous catheter;
- Implement the aseptic procedure;
- List potential complications associated with the procedure.
Purpose
- Administration of drugs via the parenteral route (antibiotics, cytostatics)
- Administration of infusion or transfusion solutionsFast supply of fluid into the bloodstream
- Long-term parenteral nutrition
Patient preparation
- Check the patient’s identity (see Fig. 13.5-4).
- Assess the patient’s clinical condition.
- Explain the procedure to the patient.
- Put the patient in the appropriate position (lying down or half-sitting).
- Adjust part of the patient’s clothing so it does not obstruct access to the site of the peripheral venous catheter.
- Ensure a suitable position of the limb for inserting an intravenous cannula.
- Select the appropriate injection site
Performing the procedure
- Check the integrity of the intravenous cannula packaging, and the expiration date.
- Wash and disinfect your hands.
- Maintain verbal contact with the patient throughout the procedure.
- Fill the connecting tubing with saline and rinse it.
- Apply a tourniquet (Esmarch tourniquet) about 15 – 20 cm above the venipuncture site. Tie the tourniquet to prevent the blood flow in the veins, but not so as to interrupt the blood flow in the arteries. Check if the radial pulse is still palpable which indicates that the blood flow through the arteries has not been interrupted.
- Place the limb in the appropriate position (below the patient’s heart); gravity slows the venous return and expands the vein; dilated blood vessels can be punctured more easily
- Palpate the injection site
- Select a suitable site for cannulation. Inadequately filled veins can be enhanced by additional measures e.g. clenching the fist, lowering the position of the limb, external heat application, etc. (see Fig. 13.5-5).

- Put on disposable rubber gloves which do not need to be sterile.
- Disinfect the injection site. In order to achieve the disinfecting effect, allow the disinfectant to dry (about 1 min.), apply disinfectant gently, the disinfected area must belarge enough; the disinfectant is applied in one direction or in circular movements from the middle of the anticipated injection site.
- It must not be touched after it has been disinfected!
- Remove the cannula from the original packaging, remove the protective cap.
- Hold the cannula with a three-point grip (between the index and middle finger of the dominant hand; the thumb fixes the bottom part of the cannula).
- Anchor the vein by pulling the skin with the thumb of your non-dominant hand; this will
also reduce the pain during penetration of the needle into the tissue.
- The needle is inserted at a 30° angle upwards; after the needle pierces the skin, tilt the needle so that it is nearly parallel to the skin, and insert it in the direction of the vein 1-2 cm deep; decreasing the angle reduces the likelihood of piercing both walls of the vein.
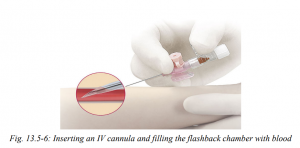
- The entry of the needle into the vain is indicated by the presence of blood in the cannula flashback chamber (see Fig. 13.5-6).
- After the puncture, quickly remove the tourniquet from the limb.
- Do not insert the needle any further but ensure the plastic part of the cannula is also in the vein.
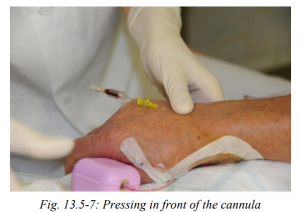
- After successful inserting the cannula into the bloodstream, place a finger over the vein above the tip of the cannula to prevent bleeding when removing the needle stylet (see Fig.13.5-7).
- Withdraw the needle stylet. Never reinsert the stylet as this can shear off the end of the cannula.
- Attach the flushed connecting tubing to the end of the inserted IV cannula (see Fig. 13.5-8) or directly using a syringe, flush the intravenous cannula with the saline prepared in the syringe.

- The cannula is carefully secured with a special sterile non-occlusive IV dressing, which prevents contamination of the injection site (see Fig. 13.5-9). Under the cannula, place a sterile gauze square (if part of the dressing) to prevent skin pressure sores while keeping the injection site dry. Each movement of the cannula leads to irritation of the vein wall and the subsequent inflammatory process which reduces the potential insertion time; fixation must not affect the blood flow around the cannula.
- The connecting tubing is fixed with a strip of tape and the end of the connecting (extension) tubing is protected with a special sterile dressing (see Fig. 13.5-10).
- Write down the date of cannula insertion (see Fig. 13.5-11).


- To administer an infusion solution, connect the tubing with the prepared infusion line.
- Always check the injection site and its surroundings before drug administration via IV cannula.
- Always flush the cannula before and after administering drugs. The flushing is done in pulses, i.e. inject 2 ml of saline solution using a syringe to the extension tubing, slow down and again quickly inject 2ml, repeat the pulse flushing and when injecting the last 2
ml of the saline solution close the connection tubing using a pean or a stopper on the tubing and attach the sterile protective cap. - If there are no signs of inflammation or other complications, the cannula can usually remain in the vein in adults up to 96 hrs, or as recommended by the manufacturer.
- The cannula replacement depends on the type and condition as well as on the condition of the injection site etc. If the protective dressing is not transparent it must be replaced after 24 hrs due to the required visual inspection of the injection site. Applying a transparent dressing on the injection site enables visual checks. The IV cannula can be redressed even after 96 hrs if the injection site does not show any signs of inflammation. The cannula dressing is often replaced simultaneously with the cannula. However, if the cannula dressing is loose, it provides insufficient protection and/or is wet, soaked with blood, then it must be replaced immediately, regardless of the date of the previous redressing. Once again, mark the date and time of the IV cannula change of dressing.
- The date and time of redressing and replacement of the cannula is also recorded in the nursing documentation.
- The cannula must be removed in the event of local complications (the injection site is painful to the touch, red, swollen).
- If there are any signs of inflammation, which may indicate systemic infection, remove the cannula and cut about 2 cm off the cannula distal end using sterile scissors and send it for a culture examination.
- Insert a new cannula at different injection site. It is recommended to alternate the limbs; the vein can be repeatedly used after 24 – 48 hrs; avoid inserting a peripheral cannula into paresthetic limbs, at the place of fracture or into rigid sclerotic veins.
___
Referensi :
- Jirkovský, D. e. (2014). Nursing Procedure and Interventions. Prague: Česká republika. doi:ISBN: 978-80-87347-16-4
- FAIX, Pavol. B Braun Echo [online]. 2002 [cit. 2011-04-06]. Intravenous cannula. Available from <http://www.bbraun.sk/bbecho/r2002/bbe_mar2002b.htm>.